

Psychiatric illness
Occupational Health Considerations
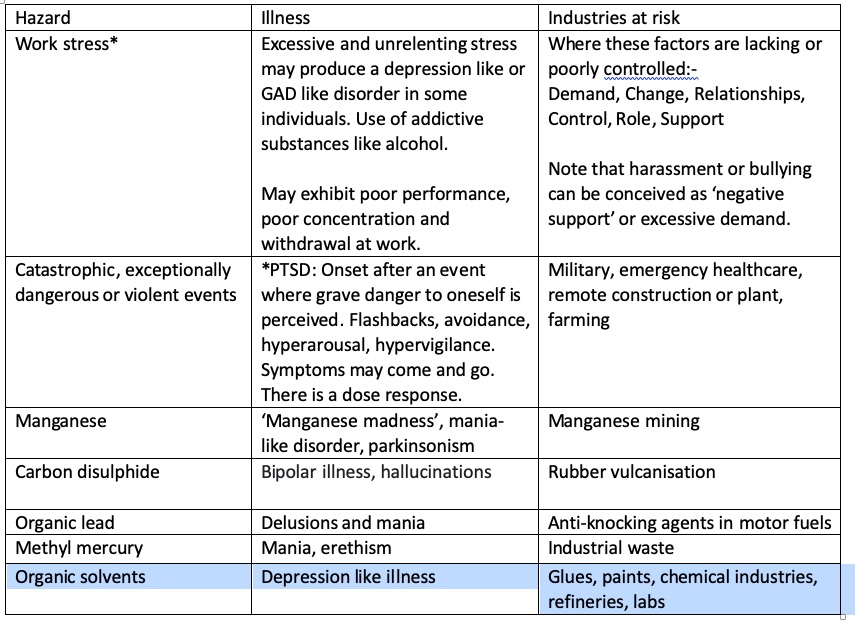
Chemical psychiatric toxins
Acute psychiatric episodes related to occupational hazards are rare but missing this diagnosis can be a grave medical error. The examining clincian should enquire about specific chemical agents such as solvents, mercury, manganese and carbon disulphide when taking an occupational history or obtain third party informants ( such as the employer) when the patient is unable to give a coherent history.
PTSD
Can be 13months (acute); >3months (chronic), or onset after 6moths (delayed). The latter is rare and should not be confused with late reporting of longer standing symptoms. Incidence in civilians exposed to violence is higher than armed forces in war theatre. Treatment is initially trauma-focussed psychotherapy by trained specialist and drug therapy as required
*Stress
Highest when risk of public failure is perceived as high. Remedial programs for stress symptoms may include sympathetic management, return to work schedule if absence has occurred, attention to Demand, Change, Relationships, Control, Role, Support within the role, psychotherapy, assistance with change management and assertiveness (in declining extra duties for example).
Clinical Aspects
My reflection